
Meet Mark, one of our UK patients who had his bariatric surgery performed with us at GB Obesitas in Malmo last year. Mark’s weight journey after the gastric bypass has been truly remarkable.
Mark Reid the music artist
Mark Reid grew up being physically active, playing football, basketball and doing track and field athletics. He had a career as a music artist together with his brothers in the group Reid (remember them? Check out their popular most songs here and here!) -life was on a roll. After the career with Reid, Mark went on to write music for other artists.
The accident and the weight gain
In 1998, at age 32, everything changed. In an everyday accident Mark falls on a slippery surface in a parking lot, lands awkwardly on his back and twists his legs in the fall. The result is damage to both knees and weeks immobilized in plaster. No more working out 2-4 times a week.
And now Mark’s life and health takes a turn for the worse. He gains weight gradually and tries “all” diets available. Nothing works. By 2012 he weighs 162 kg (equals 25 st.7lb. or 357 lb) and the self esteem is very low. The next year type 2 diabetes sets in.
Mark knows his father died early of an acute heart attack in 1992, and now fears what may be happening in the future for himself? These fears are reinforced in a doctor’s visit in 2019, where the doc bluntly states “I have seen this before. You will die early”. (This physician offers no treatment options for the obesity problem, however.)
”I’m gonna die anyway”
Shaken up, Mark turns his eyes toward the option of bariatric surgery.
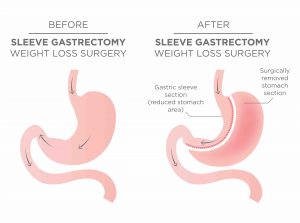
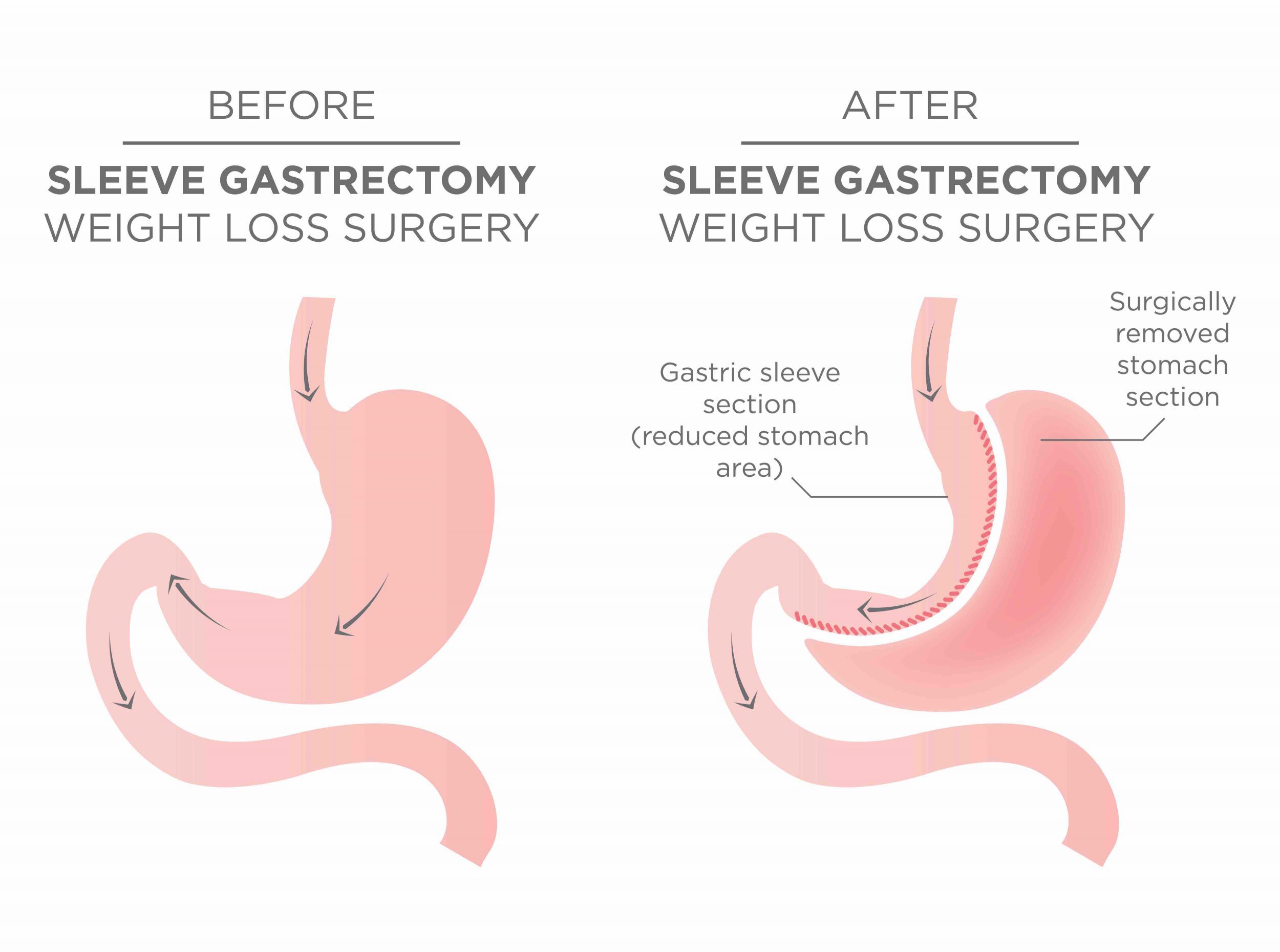
Initially he considers doing a sleeve gastrectomy in Turkey, thinking “why not risk it, I’m gonna die anyway” but hesitates as there have been many horror stories of people ending up with severe complications. Up until 2022 he celebrates every major holiday thinking it might be his last, a feeling reinforced by the passing of a good friend from an acute AMI –“am I gonna be next?”.
Then something remarkable happens. Mark stumbles upon a social media post, asking about problems with high BMI and obesity related diseases. Mark isn’t someone who normally interacts online like this, but something made him press “send” and submit his interest.
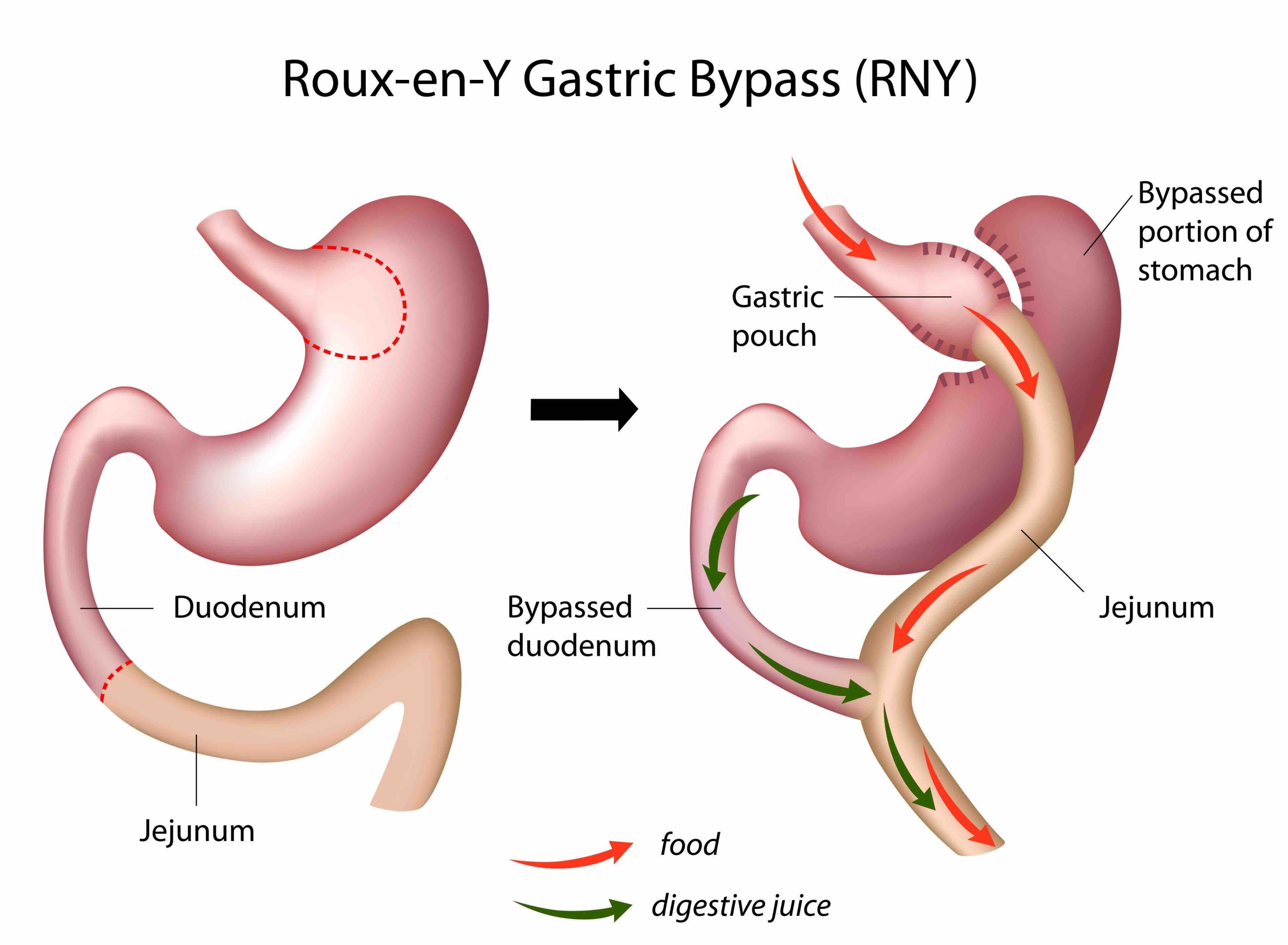
Gastric bypass in Sweden
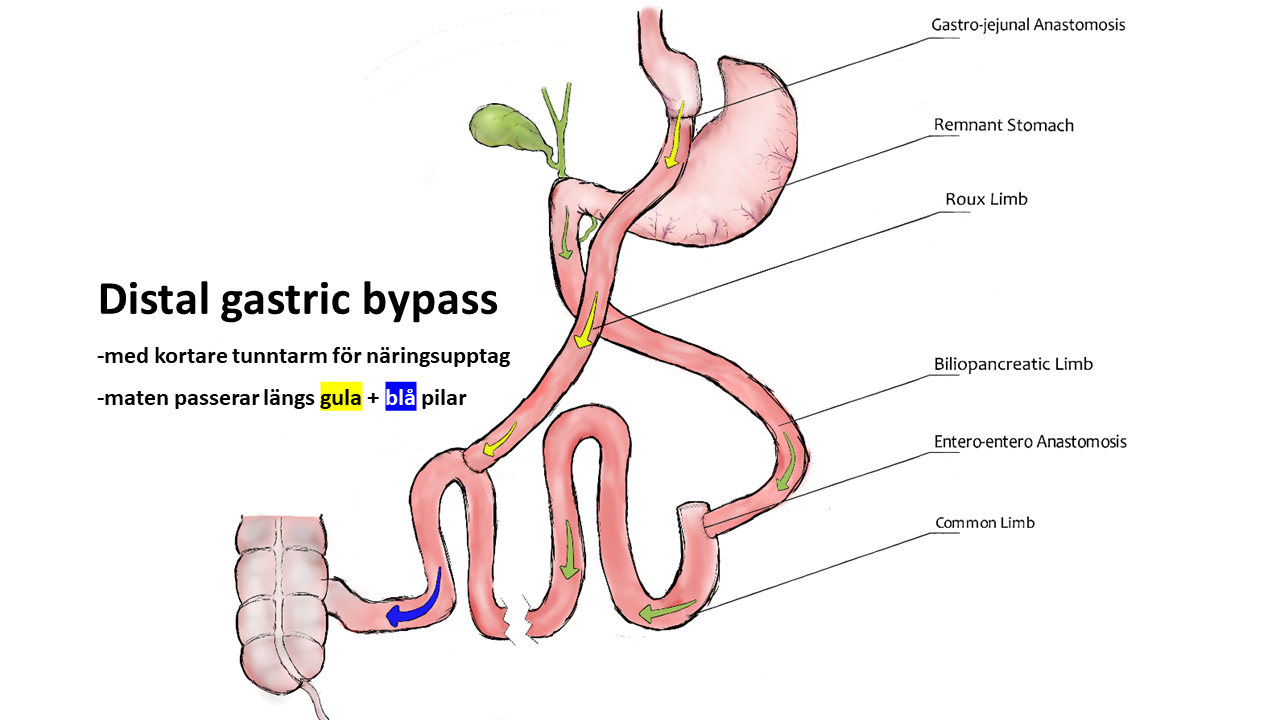
He now gets in touch with Camilla, a former patient of GB Obesitas, and gets booked to an online info meeting with Dr. Broden. The information given regarding weight gain, failed dieting, weight biology and the options of surgery “ticks all the boxes” for Mark. A gastric bypass could even reset the type 2 diabetes. “OK, I’m gonna go for it!” he decides.
So in April 2023 Mark has an online preoperative checklist meeting with Dr. Broden. They together decide upon going for a laparoscopic gastric bypass operation. Come August its time to fly into Copenhagen Airport and then take the train over the Oresund Bridge to Malmo, Sweden and the GB Obesitas clinic. The clinic is in an 1860’s building close to the water, all fully renovated to be technically modern but old style comfortable at the same time. The perioperative care was professional, smooth and the operation itself was so quick that he woke up from anaesthesia asking “is it been done already?!” (Are you considering bariatric surgery? Try our free Surgery Guide online!)
One year later -a new life begins
When we meet Mark again a year after his gastric bypass in Sweden, everything about his life has changed. He now weighs in at 111 kg (equals 17st. 6lb. or 244 lb). The metformin for type 2 diabetes is gone, as in the atorvastatin for high cholesterol. The knee problems are no more and Mark works out at least 3 times a week. He plays netball, football and plans to try volleyball. “There’s nothing I can’t do. I feel like I did in the 1980’s!”. In his new workplace working with government property contracts, they have seen the whole transformation and the comments are super positive. Mark’s self esteem is restored: “I have a new life! I am never going to give this opportunity up.”
Mark is actually correct in his feeling of having a “new life” -a large study from the Lancet shows that gastric bypass treatment in a person with obesity plus type 2 diabetes prolongs average life span with 9,3 years (and those are healthier years also).
Are you interested in how bariatric surgery with GB Obesitas works? Mark is volunteering to mentor other UK patients considering bariatric surgery. Contact us here, and we will get you in touch with Mark! If you have questions directly to Dr. Broden, just email carl@gbobesitas.com. You can learn more about our fully inclusive GBO UK Packages here. Want to have your own online info meeting in English? Just send us an email at info@gbobesitas.com .

















Senaste kommentarerna